A 48 year old with Abdominal distension
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centred online learning portfolio and your valuable comments on comment box is welcome. I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
P.Manogna
Case Report
A 48 year old male resident of chityal,
Autodriver by occupation came to the OPD with Chief complaints of:
Abdominal Distension:20days
Bilateral pedal edema: 20days
Shortness of breath: 20days
Decreased urine output:3days
Blood in stools: 3days
HOPI:
Patient was apparently asymptomatic 20days ago then he noticed abdominal distension which is insidious in onset,gradually progressive to the present size, Diffuse in nature.
B/L pedal edema which is insidious in onset, initially noticed in feet then gradually progressed up to knee, Reduces on lying down
There was Decreased urine output since 10days
Shortness of breath- insidious in onset, gradually progressive from
Grade 2 (He was unable to walk 500m which was the distance to home,after giving auto to the other person) to grade 3,According to MMRC
Blood in stools- At the end of defecation,not associated with pain
No history of abdominal pain,constipation,vomitings
No history of chest pain, palpitations,orthopnea, PND,
No history of fever, burning micturation
Past history:
Two hospital visits in past
He had a history of generalised weakness ,abdominal distension two years back for which he was diagnosed to have chronic liver failure
He received rehabilitation and he didn’t consume alcohol for 1 year and
then Started consuming alcohol ,followed by which an Episode of jaundice 1 year back with similar complaints and was managed conservatively.
K/c/o Hypertension since 10 years, initially was on T.TELMA 80 mg which was later reduced to T.TELMA 40 mg and now the patient is on T.AMLONG 5mg + ATENOLOL 50mg PO OD
N/k/c/o DM-2,TB,CAD,CVD
PERSONAL HISTORY :
Diet : Mixed
Appetite : Decreased since 20 days
Bowel and bladder movements : Decreased urine output
Sleep : Adequate
No allergies
He is alcoholic since 25 years.
250 to 300ml of whisky everyday
FAMILY HISTORY :
No history of diabetes or hypertension in the family.
GENERAL EXAMINATION :
Patient is examined in a well lit room after taking the consent.
He is conscious, coherent and cooperative.
Well oriented to time, place and person.
Pallor - absent
Icterus - present

Cyanosis - absent
Clubbing - absent
Generalized Lymphadenopathy - absent
Bilateral pedal edema - present
Pitting edema extending till the knee joint.


Vitals:
Pulse - 76 beats per minute, regular in rhythm, normal in volume and character of vessel, no radio- radial delay, no radio - femoral delay.
Respiratory rate - 20 cycles per minute
Blood pressure - 110/70 mm of hg, measured in the left arm in supine position
Temperature - afebrile
Spo2 - 98% at room air
GRBS - 94 mg/dL
Systemic examination:

Inspection - abdomen distended
Umbilicus is flat and central
No visible scars or sinuses
No visible gastric peristalsis
Palpation - No local rise of temperature
No tenderness
Organs couldn't be palpated
Percussion - fluid thrill present
Auscultation - bowel sounds normal
CVS examination:
Inspection :
Shape of chest- elliptical
No engorged veins, scars, visible pulsations
JVP - raised
Palpation :
Apex beat can be palpable in 5th inter costal space
No thrills and parasternal heaves can be felt
Auscultation :
S1,S2 are heard
no murmurs
Cns examination :
Conscious,coherent and cooperative
Speech- normal
No signs of meningeal irritation.
Cranial nerves- intact
Sensory system- normal
Motor system:
Tone- normal
Power- bilaterally 5/5
Reflexes: Right. Left.
Biceps. ++. ++
Triceps. ++. ++
Supinator ++. ++
Knee. ++. ++
Ankle ++. ++
Respiratory system:
Inspection:
Shape- elliptical
B/L symmetrical ,
Both sides moving equally with respiration .
No scars, sinuses, engorged veins
No hallowing , no crowding of ribs
Palpation:
Trachea - central
Expansion of chest is symmetrical.
Vocal fremitus - reduced on left side in mammary ,axillary and infraxillary areas
Percussion Right Left
Supraclavicular R R
Infraclavicular R R
Mammary R D
Axillary R. D
Infra axillary R D
Suprascapular R R
Infrascapular R R
Tidal percussion-resonant note
Auscultation:
bilateral air entry present. Normal vesicular breath sounds heard
Provisional diagnosis:
acute decompensation of chronic liver disease with symptoms suggestive of portal hypertension and probably due to hepatitis secondary to alcohol
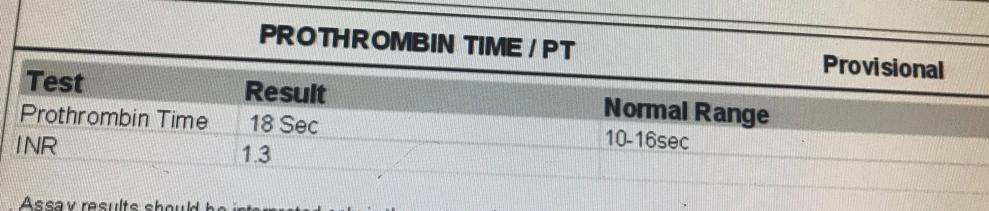
Investigations:
Ascitic tap was done




On 19/4/23









acute decompensation of chronic liver disease with symptoms suggestive of portal hypertension and probably due to hepatitis secondary to alcohol
TREATMENT :
19/4/2023
• Inj.THIAMINE 200mg in 100ml NS IV OD
• Tab.UDILIV 300mg PO BD
•Tab.ALDACTONE 50mg PO OD
• Inj.PAN 40 mg IV OD
• Tab.SPOROLAC DS PO TID
• ORS sachets - 2 sachets in 1 litre of water and 200ml after each episode
• Protein powder in a glass of milk
• Monitor vitals,input and output, Abdominal girth.
Diagnostic and therapeutic tap was done and around 800ml of ascitic fluid was drawn.
20/4/2023
Loose stools subsided
Surgery referral - in view of blood in stools
and the patient is diagnosed to have internal haemorrhoids secondary to portal hypertension,advised banding or sclerotherapy if bleed continues or if there is significant drop in haemoglobin.
21/4/2023
Endoscopy was done and diagnosed to grade 4 oesophageal varices



Comments
Post a Comment